HCPLAN GOAL STATEMENT FAQs
The Health Care Payment Learning & Action Network (HCPLAN) is committed to advancing key objectives for the health care system: higher quality, enhanced patient experience, and health equity at lower cost. The HCPLAN views adoption of two-sided risk alternative payment models (APMs) as key to these objectives and recognizes that different markets and lines of business are progressing at different rates. To that end, the HCPLAN has established new goals for adoption of two-sided risk APMs.
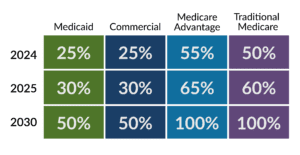
OUR GOAL STATEMENT
Accelerate the percentage of U.S. health care payments tied to quality and value in each market segment through the adoption of two-sided risk alternative payment models (Categories 3B and 4 of the HCPLAN APM Framework).
HOW ARE THE 2020 GOALS DIFFERENT FROM PRIOR HCPLAN GOALS?
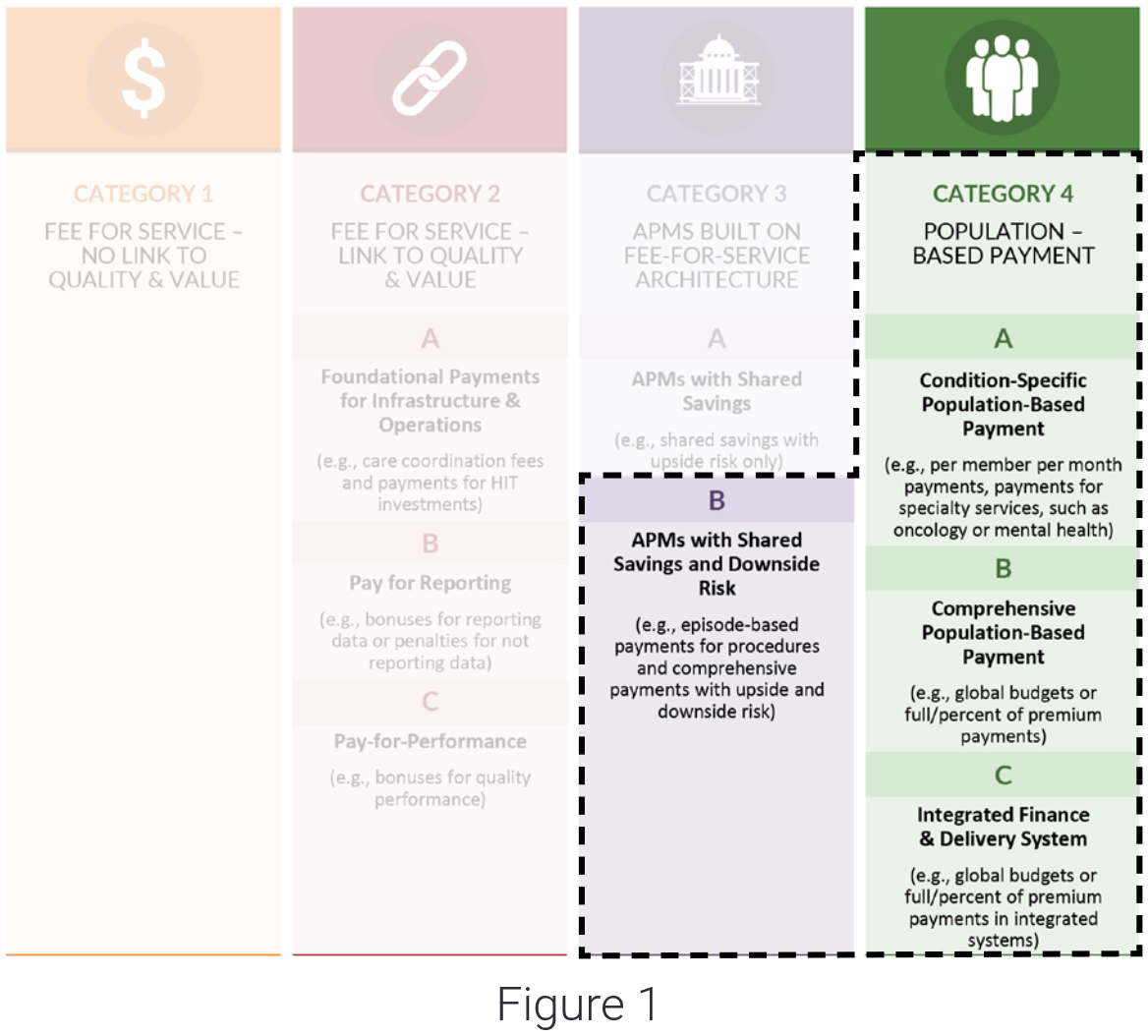
The prior HCPLAN goals were based on adoption of APMs, including APMs with shared savings (Category 3A). By contrast, the new HCPLAN goals are based on adoption of two-sided risk APMs (Categories 3B and 4) and do not include APMs with shared savings only. These categories are based on the HCPLAN APM Framework depicted in Figure 1 below.
WHAT DOES TWO-SIDED RISK MEAN?
Two-sided risk APMs are APMs that include upside gain and down-side risk, and appear in Categories 3B and 4. Two-sided APMs do not include shared-savings-only models.
WHY DID THE HCPLAN SHIFT ITS FOCUS TO ADOPTION OF TWO-SIDED RISK APMs?
Current rates of health care spending will soon become unsustainable, and there is an urgent need to substantially transform the way that health care is paid for and delivered. Two-sided risk APMs hold promise for driving this fundamental change because they promote incentives and flexibility to innovate and improve care delivery.
ARE THE HCPLAN GOALS REALISTIC, PARTICULARLY SINCE THE PREVIOUS HCPLAN GOALS WERE NOT MET?
The HCPLAN goals are ambitious but achievable if stakeholders across the public and private sectors commit to meeting them and take concerted action to do so. The boldness of the goals is commensurate with the need to transform the health care system so that it delivers better outcomes at lower costs. These goals need to be achieved, and the HCPLAN can help secure and align the commitments needed to achieve them.
HOW WILL MODELS WITH TWO-SIDED RISK APMs BE MEASURED?
Adoption of two-sided risk APMs will continue to be measured through the HCPLAN’s annual measurement effort, in which the HCPLAN invites health plans across market segments, as well as state Medicaid agencies, to quantify the amount of in- and out-of-network spending that flows through APMs. Participating plans and states categorize payments according to the HCPLAN’s APM Framework using the HCPLAN survey tool, definitions, and methodology. Two-sided risk APMs correspond to results for Categories 3B and all of Category 4, and the HCPLAN is exploring the possibility of updating the HCPLAN APM Framework to incorporate nominal risk criteria for 3B—Shared-Risk APMs.
WHY IS IT IMPORTANT TO MEASURE APM ADOPTION BY LINE OF BUSINESS?
It is important to measure APM adoption by line of business because different lines of business experience different types of challenges with APM adoption and because there is variation in rates of adoption across lines of business. Due to this variability across lines of business, the HCPLAN has set goals that are specific to each line of business to better monitor progress and identify strategies and solutions.
WHICH TYPES OF PAYMENTS WILL LIKELY BE INCLUDED FOR THE PURPOSES OF MEASURING MEDICAID PAYMENTS?
For the purposes of future measurement efforts, the Medicaid market segment will likely be similarly defined to the current measurement effort, which includes both business health plans (MCOs) have with a state to provide health benefits to Medicaid eligible individuals and state-run programs themselves. Data submitted for future surveys will also likely exclude the following: health care spending for dual-eligible beneficiaries (dual-eligible payments are reported in other lines of business), health care spending for long-term services and supports (LTSS), and spending for dental and vision services. Responses to future surveys will reflect dollars paid for medical, behavioral health, and pharmacy benefits (to the extent possible). Plans that specialize in LTSS provide unique services and may be included in future APM measurement efforts.
WHICH TYPES OF PAYMENTS WILL LIKELY BE INCLUDED FOR THE PURPOSES OF MEASURING TRADITIONAL MEDICARE PAYMENTS?
For the purposes of future measurement efforts, the APMs CMS will use to calculate the percent of payments made through categories 3B and 4 of the APM Framework will include APMs that qualify as Advanced Alternative Payment Models (AAPMs). The most recent CMS Office of the Actuary (OACT) annual Part A and B expenditure data are used to calculate the denominator and are obtained directly from OACT. However, the future survey will explore whether excluding certain part A and B spending that is not readily linked to AAPMs is appropriate, such as Federally Qualified Health Centers and rural health clinics.



 Emily DuHamel Brower, M.B.A., is senior vice president of clinical integration and physician services for Trinity Health. Emphasizing clinical integration and payment model transformation, Ms. Brower provides strategic direction related to the evolving accountable healthcare environment with strong results. Her team is currently accountable for $10.4B of medical expense for 1.6M lives in Medicare Accountable Care Organizations (ACOs), Medicare Advantage, and Medicaid and Commercial Alternative Payment Models.
Emily DuHamel Brower, M.B.A., is senior vice president of clinical integration and physician services for Trinity Health. Emphasizing clinical integration and payment model transformation, Ms. Brower provides strategic direction related to the evolving accountable healthcare environment with strong results. Her team is currently accountable for $10.4B of medical expense for 1.6M lives in Medicare Accountable Care Organizations (ACOs), Medicare Advantage, and Medicaid and Commercial Alternative Payment Models. Mr. James Sinkoff is the Deputy Executive Officer and Chief Financial Officer for Sun River Health (formerly known as Hudson River HealthCare), and the Chief Executive Officer of Solutions 4 Community Health (S4CH); an MSO serving FQHCs and private physician practices.
Mr. James Sinkoff is the Deputy Executive Officer and Chief Financial Officer for Sun River Health (formerly known as Hudson River HealthCare), and the Chief Executive Officer of Solutions 4 Community Health (S4CH); an MSO serving FQHCs and private physician practices. Victor is the Chief Medical Officer for TennCare, Tennessee’s Medicaid Agency. At TennCare, Victor leads the medical office to ensure quality and effective delivery of medical, pharmacy, and dental services to its members. He also leads TennCare’s opioid epidemic strategy, social determinants of health, and practice transformation initiatives across the agency. Prior to joining TennCare, Victor worked at Evolent Health supporting value-based population health care delivery. In 2013, Victor served as a White House Fellow to the Secretary of Health and Human Services. Victor completed his Internal Medicine Residency at Emory University still practices clinically as an internist in the Veteran’s Affairs Health System.
Victor is the Chief Medical Officer for TennCare, Tennessee’s Medicaid Agency. At TennCare, Victor leads the medical office to ensure quality and effective delivery of medical, pharmacy, and dental services to its members. He also leads TennCare’s opioid epidemic strategy, social determinants of health, and practice transformation initiatives across the agency. Prior to joining TennCare, Victor worked at Evolent Health supporting value-based population health care delivery. In 2013, Victor served as a White House Fellow to the Secretary of Health and Human Services. Victor completed his Internal Medicine Residency at Emory University still practices clinically as an internist in the Veteran’s Affairs Health System. Dr. Brandon G. Wilson, DrPH, MHA (he, him, his) joined Community Catalyst as the Director of the Center for Consumer Engagement in Health Innovation, where he leads the Center in bringing the community’s experience to the forefront of health systems transformation and health reform efforts, in order to deliver better care, better value and better health for every community, particularly vulnerable and historically underserved populations. The Center works directly with community advocates around the country to increase the skills and power they have to establish an effective voice at all levels of the health care system. The Center collaborates with innovative health plans, hospitals and providers to incorporate communities and their lived experience into the design of systems of care. The Center also works with state and federal policymakers to spur change that makes the health system more responsive to communities. And it provides consulting services to health plans, provider groups and other health care organizations to help them create meaningful structures for engagement with their communities.
Dr. Brandon G. Wilson, DrPH, MHA (he, him, his) joined Community Catalyst as the Director of the Center for Consumer Engagement in Health Innovation, where he leads the Center in bringing the community’s experience to the forefront of health systems transformation and health reform efforts, in order to deliver better care, better value and better health for every community, particularly vulnerable and historically underserved populations. The Center works directly with community advocates around the country to increase the skills and power they have to establish an effective voice at all levels of the health care system. The Center collaborates with innovative health plans, hospitals and providers to incorporate communities and their lived experience into the design of systems of care. The Center also works with state and federal policymakers to spur change that makes the health system more responsive to communities. And it provides consulting services to health plans, provider groups and other health care organizations to help them create meaningful structures for engagement with their communities. Tamara Ward is the SVP of Insurance Business Operations at Oscar Health, where she leads the National Network Contracting Strategy and Market Expansion & Readiness. Prior to Oscar she served as VP of Managed Care & Network Operations at TriHealth in Southwest Ohio. With over 15 years of progressive health care experience, she has been instrumental driving collaborative payer provider strategies, improving insurance operations, and building high value networks through her various roles with UHC and other large provider health systems. Her breadth and depth of experience and interest-based approach has allowed her to have success solving some of the most complex issues our industry faces today. Tam is passionate about driving change for marginalized communities, developing Oscar’s Culturally Competent Care Program- reducing healthcare disparities and improving access for the underserved population. Tamara holds a B.A. from the University of Cincinnati’s and M.B.A from Miami University.
Tamara Ward is the SVP of Insurance Business Operations at Oscar Health, where she leads the National Network Contracting Strategy and Market Expansion & Readiness. Prior to Oscar she served as VP of Managed Care & Network Operations at TriHealth in Southwest Ohio. With over 15 years of progressive health care experience, she has been instrumental driving collaborative payer provider strategies, improving insurance operations, and building high value networks through her various roles with UHC and other large provider health systems. Her breadth and depth of experience and interest-based approach has allowed her to have success solving some of the most complex issues our industry faces today. Tam is passionate about driving change for marginalized communities, developing Oscar’s Culturally Competent Care Program- reducing healthcare disparities and improving access for the underserved population. Tamara holds a B.A. from the University of Cincinnati’s and M.B.A from Miami University.


 Dr. Peter Walsh joined the Colorado Department of Health Care Policy and Financing as the Chief Medical Officer on December 1, 2020. Prior to joining HCPF, Dr. Walsh served as a Hospital Field Representative/Surveyor at the Joint Commission, headquartered in Oakbrook Terrace, Illinois.
Dr. Peter Walsh joined the Colorado Department of Health Care Policy and Financing as the Chief Medical Officer on December 1, 2020. Prior to joining HCPF, Dr. Walsh served as a Hospital Field Representative/Surveyor at the Joint Commission, headquartered in Oakbrook Terrace, Illinois.








